Cancers of the pleura
Primary tumor (mesothelioma) is a rare, and secondary tumors are common. Mesothelioma can be benign or malignant more often. Malignant pleural diseases more common in individuals chronically exposed to asbestos. Secondary tumors arise from cancer of the bronchus, stomach, liver and other facilities. Malignant lesions in the pleura lead to hemorrhagic pleural effusion.
pneumothorax
The presence of air in the pleural cavity is known as pneumothorax. Pneumothorax can be spontaneous, traumatic, and iatrogenic (artificially). Another classification is to divide them into the open, closed, and the error pneumothorax (tension pneumothorax). In an open penumothorax a free rental on the surface of the lungs through which air is obtained from the pleural cavity during inspiration and expiration. In a closed pneumothorax, pleura can not communicate with the outside. In tension pneumothorax, there is a mistake the slot on the surface of the lungs through which air enters the pleural cavity, but can not escape. As a result, tension pneumothorax develops, leading to respiratory and cardiac embarrassment.
of a spontaneous pneumothorax : The result of rupture of pulmonary lesions leading to leakage of air into the pleura. Subpleural blebs or bullae, pulmonary tuberculosis, congenital cystic disease of the bronchi, chronic bronchitis with emphysema, bronchial asthma, pneumoconiosis, and Staphylococcal pneumonia are common medical causes. Fracture of the ribs, thoracotomy, lung puncture on a needle biopsy, and bronchial rupture are common surgical causes. Sometimes a pneumothorax is produced artificially for diagnostic radiology in lung or as therapy to arrest massive nehoptysis.Pluća fails to hilium, when air enters the pleura and abolishes the negative pressure.
Clinical features : attack with unilateral pleuritis dispneja.Osjećaj pain and something gave way, was blamed by many, shortness of breath and an unproductive cough to develop soon. In tension pneumothorax respiratory embarrassment and cyanosis may be noted vidljivo.Zahvaćene hand and it does not move with breathing. Mid-line tructures is shifted to the opposite side. Percussion note hyper-resonant. Breath sounds are absent in many cases. If air enters the pleural cavity as in tension pneumothorax and open pneumothorax amphoric breath sounds čuti.Posebna percussion phenomenon "coin sound". The money is kept securely These front of the chest is struck with the second money. Auscultation on the back side of the chest reveals a metallic note. Adventitous sounds like the clicking sounds synchronous with the heart can be heard in the left-sided pneumothorax. Differential diagnosis includes pneumothorax other painful conditions associated with dyspnea, such as myocardial infarction and pulmonary infarction. Severe emphysema, large bullae, and diaphragmatic hernia can cause problems in diagnosis.
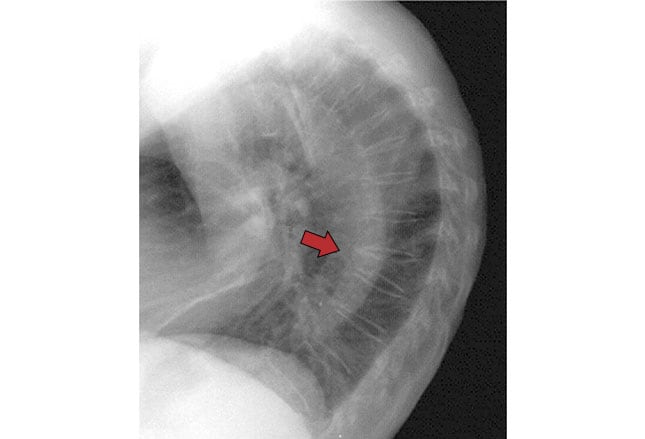
Radiological features : radiological features are diagnostic of a well-developed slučaj.Zahvaćene hypertranslucent by the due collection of free air in the pleural cavity and the absence of normal lung markings. Outside the borders collapsed lung is seen as a sharp margin on the background air. There is a shift of the trachea and mediastinum to the opposite side. Chest X should be in an upright posture, so that even a small collection of air will not be missed.
Complications : Although in most cases, spontaneous pneumothorax is a simple, serious complications can develop in some cases. These are:
1st Severe cardio-respiratory embarrassment due to compression of normal lung, which displaced the mediastinum in cases of tension pneumothorax
2nd air embolism
3rd surgical emphysema
4th infection of the pleural cavity resulting in the formation of hydro-or pyo-pneumothorax;
5th Penumothorax on the opposite side of the pre-existing lung disease and
6th failure of the spread collapsed lung.
HydroPneumothorax
When both air and liquid are present in the pleural cavity, it is known as hydropneumothorax. This is usually the result of rupture of pulmonary lesions, leaving the air, and exudates in the pleural cavity. In many cases, it is caused by tuberculosis. Other causes include lung abscess, bronchiectasis, bronchogenic carcinoma, and trauma to the chest. Some cases of pneumothorax is converted to hydro-pneumothorax, when the discharge develops as a result of infection.
The hydro-pneumothorax, a higher level of horizontal fluid can cause numbness to show what moves you pateint was made to adopt a different position (shifting dullness). On shaking gently until the patient auscultating the air-liquid interphase, succussion splash is heard. Chest readiograph reveals horizontal upper level of the liquid with the findings of pneumothorax above it.
Management of pneumothorax
Small closed pneumothorax, which did not seriously symptomatic may remain alone with bed rest and analgesics. Since the air will be absorbed within a few days. Tension pneumothorax can present as life-threatening emergency. If the tension is relieved to let the air May a patient die of cardio-respiratory failure.
Emergency Management : let the air by inserting a needle into the second intercostal SCAE 2-3cm beyond the lateral border of sternum and is connected to a rubber tube which was led under water, in order to prevent re-entry of air (underwater seal). This procedure can be initiated outside the hospital in time. Often, the needle has a tendency to block and intrapleural pressure goes up. Injury to the lung surface, bleeding into the pleura, infection and surgical emphysema, and other harmful side effects. When pneumothorax reaccumulates blockade pins, May he be replaced by wider tires catheter. After removing the patients in the hospital, the ideal procedure for the establishment of the pleura drainage hose connected to an underwater pečat.Cijev must be in place for several days or weeks. Antibiotics are given to prevent secondary infection of the pleura. It is obviously an underlying condition is treated with certain medications. The recovery of lung function is facilitated by starting physiotherapy at an early stage. If the lung does not expand with the removal of air, vacuum pleural cavity can help. Surgical repair of the pleural surface may be needed in intractable cases.

0 comments:
Post a Comment